Editorially Independent Content
Comparing the three technologies used in Anterior Segment Imaging.
Based on an ASCRS presentation by Mitch Weikert, MD, from Baylor College of Medicine.
Anterior Segment Imaging is very important to our clinical practice and, as the technology advances, it’s becoming even more vital to providing the best possible service to our patients.
There are three principal technologies we use in Anterior Segment Imaging: Placido Imaging, Scheimpflug Imaging and Optical Coherence Tomography or OCT.
With Placido Imaging, which is a reflective technology, we have a device with concentric rings of light that are projected onto the cornea and the reflection is imaged. (See Figure 1.)
Figure 1
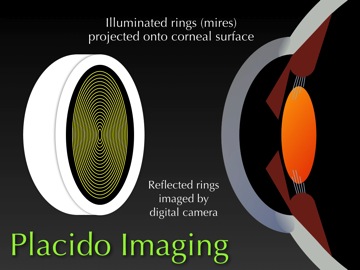
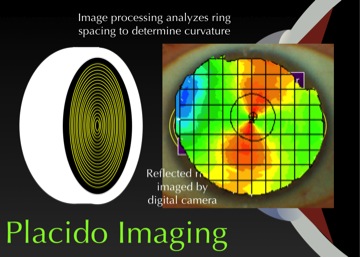
Image processing software then analyzes the spacing between the rings to determine the cornea’s shape. Where the rings are closer together, the cornea is steeper or more curved. Where the rings are farther apart, the cornea is flatter or less curved. Using mathematical algorithms, the processing software converts that spacing or those dimensions to generate maps that illustrate the shape of the cornea. (See Figure 2.)
Figure 2
Placido Imaging has advantages as well as disadvantages. Since there are many rings and many points on those rings, one advantage is that Placido Imaging provides very accurate measurements of curvature. It can measure within an eighth of a diopter on artificial corneas and within a quarter diopter on human corneas.
Placido Imaging also gives additional information about surface quality. For example, you can look at the image of the rings and determine whether or not the surface is smooth or irregular. (See Figure 3.)
Figure 3
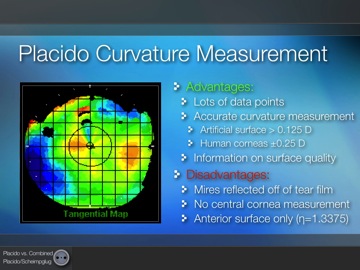
With Placido Imaging, the mires or rings reflect off the tear film. If you have poor tear film or an irregular surface, one disadvantage is that you’re going to get poor data or measurements. Also, since you can’t have a circle with an infinitely small radius, you can’t measure the central part of the cornea directly. And with Placido Imaging, you can only measure the anterior surface of the cornea.
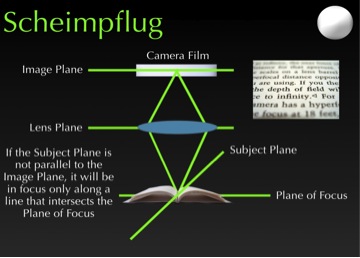
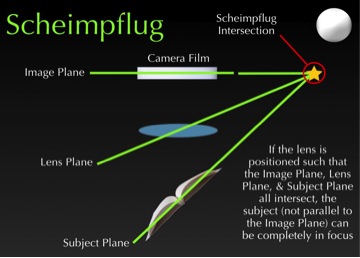
This brings us to the next technology, Scheimpflug Imaging, which can be a bit tricky to explain but bear with me. In conventional photography, the plane of the camera is parallel to the plane of the lens, which is parallel to the plane of the target. When imaging the eye, if the subject is parallel to the camera and film, we get a good 2-dimensional coronal image of the front of the eye. (See Figure 4.)
Figure 4
If that subject is slightly tilted, we’re going to have parts of that subject that are going to be away from the center of the image and therefore out of focus. But if we tilt the lens such that the lens plane intersects the film plane, which also intersects the subject plane—at a point we call the Scheimpflug intersection—something phenomenal happens. We get a cross-sectional image of the eye. (See Figure 5.)
Figure 5
If we extrapolate this data in relation to the eye, we get an image that divides the eye in a way that gives us a cross-sectional image of that eye. The image processing software then analyzes those images and computes curvatures and dimensions of the front of the eye.
Scheimpflug Imaging also has its advantages and drawbacks. The advantages are that there are thousands upon thousands of elevation points. We’re able to measure the center part of the cornea as well as both the anterior and posterior surfaces of the cornea.
Since Scheimpflug technology is optically based, one disadvantage it poses is that it can’t penetrate the iris, allowing us to image the cilliary sulcus. Because of this, we have to compare this elevation data to a reference surface, which can introduce error. We also need extremely high resolution to measure the center of the cornea where we have extremely subtle differences in height.
That brings us to the third technology for Anterior Segment Imaging—Optical Coherence Tomography or OCT—which is based on the principle of interferometry. With OCT, we have a light source that has a beam that hits a beam splitter. (See Figure 6.) It then goes up to a reference mirror and reflects back to our detector. That is our reference arm that tells us the distance that light has traveled.
Figure 6
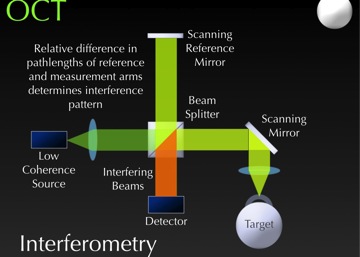
In the measurement arm, the light passes through the beam splitter and is reflected onto our target, in this case, the eye. The light bounces back as well as travels to our detector.
When these events happen simultaneously—where the light comes together and hits the detector—we get interference. The device then mathematically computes different reflection points in the eye to image the anterior segment.
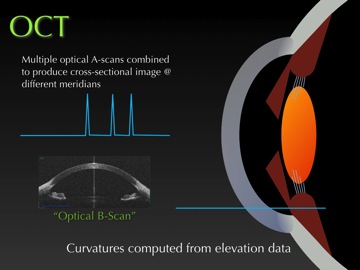
As we image different points across the eye, we essentially get a series of Optical A-scans. When multiple A-scans are combined, they produce an Optical B-scan, which is a cross-sectional image where the curvature is computed from elevation data at different meridians. (See Figure 7.)
Figure 7
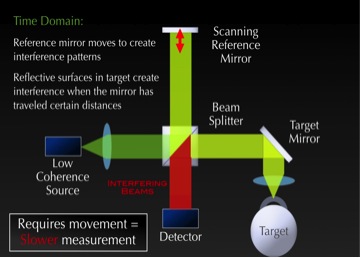
There are two types of OCT technology: Time Domain OCT and Frequency or Spectral Domain OCT. In Time Domain OCT, the reference arm varies by moving a scanning mirror.
By varying the length of the reference arm, we can choose where we interfere with the signal that comes back from the eye. This allows us to select different depths of the eye to image. Since this requires movement of that reference mirror, it’s a slower process so the resolution is slightly lower. (See Figure 8.)
Figure 8
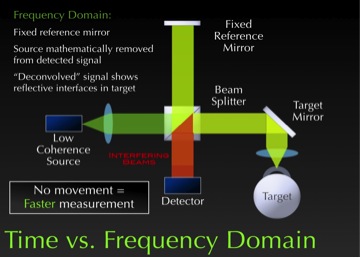
With Frequency or Spectral Domain OCT, the mirror is fixed so the reference arm doesn’t move. This system works by mathematically removing the reference signal from the detected signal and the interference pattern.
In doing so, it can remove the source signal and detect the different reflective interfaces coming from the eye. It then puts those together to determine the shape and image of the eye. (See Figure 9.)
Figure 9
Since Time Domain OTC is a slightly lower resolution, it’s used more for imaging applications, like CTs or MRIs of the eye, where you’re able to look at structures within the eye.
While Frequency Domain OCT also images structures within the eye, it generally images a smaller area. But, since it has higher resolution, it can do a better job measuring the shape of the eye. We can use it to measure the shape and power of the cornea and then use that data in applications where we need numerical values, such as IOL calculations and refractive surgery.
In conclusion, to fully utilize these Anterior Segment Imaging technologies effectively, it pays to really understand their underlying principles and unique capabilities. When we know what they do well, and what they don’t do well, this knowledge ensures that we get valuable information that can be used in a judicious manner to benefit our clinical practices and patients.




